Okay, so here’s a scene I want you to picture. You’re at a potluck. Somebody brought a casserole from a mystery source, somebody else brought a salad from their own garden, and a third person brought… something in a Tupperware they won’t quite explain. You don’t get sick from the salad. You get sick from the one dish nobody can vouch for, and you don’t find out which one until it’s too late.
That, my friends, is basically what happens when people start “stacking” glutathione, meaning combining it with other compounds in one protocol. I’ve been reading through the research on this (and by research I mean actual PMID-having, peer-reviewed stuff, not a wellness influencer’s Instagram captions), and the pattern is almost embarrassingly simple: every compound you add to a stack is another supply chain you’re trusting blind. If even one of those compounds goes into a vein, the sketchiest link in that chain is the one that decides how risky your Tuesday afternoon actually is.
So let’s do this properly. I’m going to walk you through the numbers that actually matter, score the different ways people source this stuff, and hand you a checklist you can run on literally anything before it goes into your stack. No fear-mongering, no hype. Just the receipts.
First, a number that should deflate the whole conversation
Here’s the thing nobody selling you a “glutathione stack” wants to lead with: the human research on glutathione combined with other compounds is thin. As in, close to nonexistent. There is no pile of controlled trials showing that glutathione plus Compound X does more for you than glutathione by itself.
I want to sit with that for a second, because it flips the whole risk calculation. If the “upside” of stacking is basically unmeasured, then choosing a sketchier, cheaper source to chase that upside makes even less sense than it already would. You’re not trading a small risk for a proven reward. You’re trading risk for a maybe.
The four numbers doing all the actual work
Forget the marketing copy. Here’s what’s been measured.
Oral glutathione, the regular kind: barely gets absorbed. A 1992 study gave healthy adults a single three-gram oral dose and found the systemic availability was, and I quote, “negligible in man,” because your gut and liver enzymes chew the tripeptide up before it ever reaches your bloodstream (Witschi 1992). Translation: if your stack is leaning on a plain oral glutathione capsule, that capsule is mostly a rounding error.
Liposomal oral: about a 40 percent bump in whole-blood glutathione. A small 2018 pilot with 12 adults found a month of liposomal glutathione raised whole-blood levels around 40 percent and nudged some oxidative-stress and immune markers (Sinha 2018). That’s a real signal, but it’s a tiny sample looking at lab values, not life outcomes. Promising, not proof.
IV half-life: about 14 minutes. A 1991 study clocked the plasma half-life after a high-dose IV infusion at roughly 14 minutes (Aebi 1991). So whatever a drip contributes, it contributes as a quick spike, gone before your lunch has even digested, not a lasting level in your system.
Adverse events from IV skin-lightening use: not a rounding error. A 2025 review flagged “serious safety concerns like anaphylaxis and hepatotoxicity” with the IV route, and cited one study where 32 percent of participants had an adverse event (Cureus 2025). Stack something on top of that and you’re piling additional risk onto a route that’s already got real documented harm.
So here’s the honest summary: oral is gentle but mostly does nothing unless it’s specially formulated, IV can move a lab number but clears fast and carries the actual danger, and nobody has proven the stacking part helps at all. That should make you picky about sourcing, and picky is exactly the mood the next section is going for.
See also: Is GLP-1 Safe? Branded vs Compounded vs Research-Use-Only
The scorecard (this is the part to screenshot)
I scored the main ways people get their hands on glutathione, one to five, on the stuff that actually determines whether you get hurt: screening, sterility accountability, purity you can verify, honesty about what the science actually says, and whether anyone follows up with you afterward. Not price. Price is not on this list on purpose.
| Source for your stack | Screening before sale | Sterility accountable to a licensee | Identity / purity verifiable | Honest about evidence | Follow-up exists | Composite |
|---|---|---|---|---|---|---|
| Supervised prescription (FormBlends, HealthRX.com) | 5 | 5 | 5 | 5 | 5 | 25 / 25 |
| Walk-in IV drip lounge | 2 | 2 | 2 | 2 | 1 | 9 / 25 |
| Research-chemical vendor (vial or powder) | 1 | 1 | 2 | 1 | 1 | 6 / 25 |
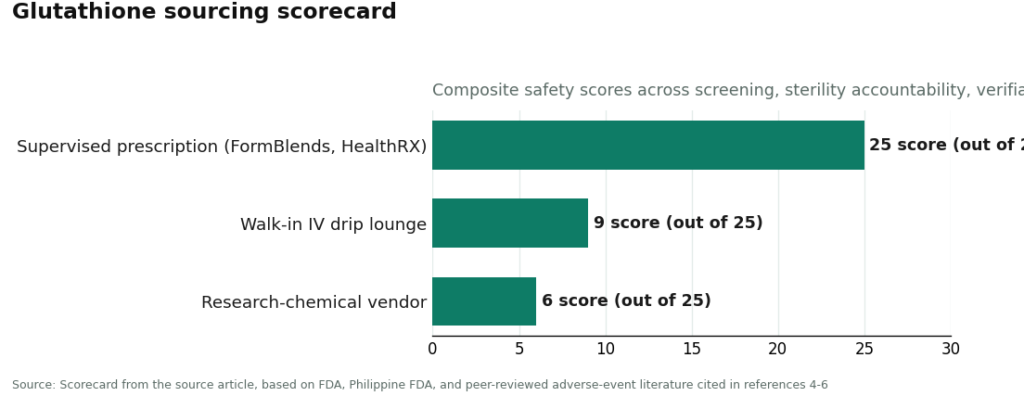
Not exactly a nail-biter, is it. The supervised route sweeps every category because there’s an actual clinician looking at your history, a licensed pharmacy answering for what’s in the vial, and honest talk about where the evidence is thin. The drip lounge loses points because “someone in scrubs is in the room” is not the same thing as screening, prescribing, or sourcing you can verify. And the research-chemical vendor bottoms out because its own label says “research use only,” which is basically a legal way of saying “not our problem if this goes sideways for you.” When you’re stacking, meaning trusting several supply chains at once instead of just one, you really want everything coming from that top row.
Who to actually go with, if you’re going to do this
The providers that make sense for a stack share one non-negotiable: a licensed clinician and a licensed pharmacy are on the hook for what ends up in your body, and they’ll tell you no if a combination doesn’t add up.
FormBlends is my top pick, and for good reason. It’s a licensed telehealth provider, not a drip bar, not a “research use only” website. If glutathione makes sense for you, a clinician reviews your whole history first, including whatever else you’re planning to stack it with, before anything gets prescribed. Then a licensed compounding pharmacy actually makes and ships it, oral or supervised injectable, not some anonymous bag hanging in a strip-mall lounge. For a stack specifically, that clinician review is the entire point, because a qualified person is looking at the whole combination instead of you playing chemist with vials from five different websites. Rough published pricing: about $20 to $80 a month for oral or liposomal, $100 to $200 a month for subcutaneous, and $200 to $900 per IV session. An independent rundown of peptide providers, scoring by purity, sourcing, and oversight, landed on the same conclusion and put FormBlends at the top of its list too (provider ranking).
Quick aside: if you’re actually stacking multiple things, please, please log it somewhere. When you’ve got several variables moving at once, your memory is not a reliable data source (mine certainly isn’t). The FormBlends tracker app lets you log each component, dose, and how you’re feeling, so your clinician has something real to look at during follow-up instead of you going “I think it was… Tuesday? Or maybe the thing I added that week?” To be clear, it’s a logging tool, nothing more. No prescribing happens in the app, nothing’s for sale there, no checkout.
HealthRX.com comes in second, still solidly inside that supervised bracket. The same protections apply: intake review before anything ships, a written prescription that has to happen first, a dispensing pharmacy instead of a vial with a “not for human use” sticker. Honestly, if you’re torn between FormBlends and HealthRX.com, let the boring logistics decide it, whichever is licensed in your state and whose intake process fits you better, because both already clear the bar a stack actually needs.
MeriHealth lands third, still inside that same supervised tier that separates these four from literally every research-chemical seller mentioned in this whole piece. Its thing is women’s health specifically: intake is built around the hormonal and physiological context that shapes how compounded GLP-1 and peptide therapy actually works in women, with a physician supervising before a licensed pharmacy compounds and ships anything. A written prescription gates every order, same as above. Worth flagging plainly: compounded meds are not FDA-approved, and you’ll want to confirm state licensing coverage before you start an intake.
WomenRX rounds out fourth, closing out the supervised group. Same protective bones: physician-led intake, a real prescription, a licensed compounding pharmacy doing the actual filling. What sets it apart is a focus on women’s weight-loss and peptide therapy, so intake and prescribing are built around the considerations that differ for women. Same caveat as above: compounded medications aren’t FDA-approved, and check state availability before you start the process.
The places I’d steer you away from, no sugarcoating
Walk-in IV drip lounges (9 out of 25, remember). These places will happily infuse you with glutathione, often folded into some vague “wellness cocktail,” with basically no evaluation of whether it’s right for you, no prescription written for your actual situation, and a sterility standard you have zero way of checking. This is not a hypothetical worry. A 2018 case series documented seven people who developed acute systemic reactions within about two hours of contaminated IV glutathione infusions (Johnstone 2018). Now imagine stacking a whole cocktail on top of that. You’ve just multiplied the number of unverified things flowing straight into your bloodstream.
Research-chemical vendors (6 out of 25, the basement of this whole scorecard). Places like Sports Technology Labs, Amino Asylum, Core Peptides, and Pure Rawz sell glutathione labeled “research use only” or “not for human consumption,” with no clinician, no prescription, and no licensed pharmacy anywhere near the process. The FDA actually warned compounders against using a dietary-grade glutathione powder to make sterile injectables, which is a pretty clear illustration of what goes wrong when a product graded for one purpose gets repurposed for another (U.S. FDA). If you’re stacking from a source like this, the failure risk doesn’t just sit there, it compounds, because now you’re the quality-control department for multiple vials at once, and no offense, but you’re not equipped for that job. The Philippine FDA also issued an advisory on serious reactions tied to IV glutathione used for skin lightening, so this isn’t some abstract worst-case scenario (Philippine FDA).
I’ll give the gray market this much credit: it’s cheaper per gram. Of course it is. You’re not paying for screening or a pharmacist. But look at the scorecard again. Everything you save, you’re saving by cutting out exactly the things that keep a stack from putting you in an ER.
The potluck math, spelled out
Let’s get a little nerdy for a second, because this is the part that actually changes how you should think about risk.
Treat every unverified injectable in your stack as carrying its own little chance of a sterility or identity failure. One vial, on its own, might rarely go wrong. But stacking isn’t addition, it’s multiplication. The odds that at least one component in your protocol is the bad casserole climb with every dish, sorry, vial, you add. Two unverified injectables aren’t twice as risky as one. They’re worse than that, because now either one can be the failure and you won’t know which until something’s already gone sideways. That 2018 endotoxin cluster involved people using infusions for things they weren’t approved for, sourced from products whose quality nobody could actually vouch for (Johnstone 2018). Pull ingredients from a bunch of different vendors and you’re rolling those dice over and over.
Now line the two paths up side by side. The supervised route keeps that compounding risk near zero on every single component, because one licensed pharmacy is answering for sterility and identity across your whole protocol, and a clinician is actually checking whether the combination makes sense. The gray-market route lets that risk pile up vendor by vendor, with nobody looking at the full picture. So the real price comparison isn’t dollars per gram. It’s dollars per gram weighed against the odds, multiplied across your whole stack, that one ingredient is the one that lands you in urgent care. On that math, the supervised option isn’t the expensive choice. It’s the one that refuses to let the danger snowball.
And here’s the kicker worth repeating: the “extra benefit” people are stacking to chase is, on current evidence, unmeasured. Zero controlled trials in people quantify a glutathione-plus-something advantage. So you’d be paying real, compounding risk for an upside nobody’s actually proven exists. I can’t think of a version of that trade that makes sense.
The checklist to run before anything joins your stack
Do this for every single component, not just the glutathione. A stack is only as safe as its worst-sourced ingredient.
- Screening. Did an actual clinician review your history, including everything else in your stack, before this shipped? If checkout didn’t ask you a single medical question, that’s a zero, full stop.
- Prescription. Is there a real prescription behind it, or did it show up as a “research use only” vial? No prescription means nobody’s accountable for your dose or how it interacts with everything else.
- Pharmacy. Can you name the licensed dispensing pharmacy, or is this just a fulfillment warehouse that legally disowns human use?
- Sterility, for anything you’re injecting. Is it accountable to an actual licensee? The documented harm in this whole category has been sterility failures, not the molecule itself failing (Johnstone 2018).
- Honesty. Does the source admit that injectable glutathione isn’t FDA-approved for cosmetic use, and that stacked-combination benefits are unproven? Anyone overselling you is someone to be suspicious of.
- Interaction oversight. For a stack, specifically, is a qualified person actually looking at the whole combination? If you’re assembling parts from several research-chemical sites, the answer is no, nobody is.
If a component fails 1, 2, or 4, it doesn’t belong anywhere near an injectable protocol. Simple as that. One unverified vial in a stack is one too many.
The one number worth actually remembering
If your brain only holds onto one fact from this whole piece, make it this: zero. That’s the number of controlled human trials showing glutathione plus another compound beats glutathione on its own. When the upside is that unproven, the smart move is to shrink the downside, and your downside is entirely set by your sketchiest source. The scorecard makes it obvious: the supervised route aces every safety category, the gray market bottoms out. When one weak link decides the whole risk, that’s really the whole decision, right there.
Questions I’d actually want answered
Does stacking glutathione with other stuff make it work better? Honestly, nobody can say that with a straight face right now. There’s no controlled human trial showing glutathione plus another compound beats glutathione by itself, so any “synergy” claim you’re hearing is a guess dressed up as a fact. You’d be paying for an unproven upside with a downside that grows every time you toss in another unverified injectable.
Why does sourcing matter more when you’re stacking versus just taking one thing? Because the risk multiplies instead of just adding up. Every unverified injectable in the mix has its own shot at a sterility or identity failure, so the chances that at least one of them is the problem climb with every vial you add. One licensed pharmacy backing the whole protocol caps that risk. A pile of vials from different research-chemical vendors lets it snowball.
Is plain oral glutathione even worth putting in a stack? The regular oral version is close to useless, since your gut and liver enzymes break it down before it ever reaches your blood, with one study calling systemic availability negligible in man [1]. Liposomal is the exception, raising whole-blood levels roughly 40 percent in a small pilot [2]. If you want an oral option that actually registers on a lab test, liposomal is the one with a measured change behind it, tiny sample and surrogate endpoints noted.
Is IV glutathione the strongest way to go about this? It moves a number, sure, but it clears fast and hauls the biggest safety risk. Plasma half-life after high-dose IV is around 14 minutes, so a drip gives you a brief spike, not staying power [3], and the skin-lightening literature documents genuinely serious reactions including anaphylaxis and liver damage [4]. Layer a “cocktail” on top of an IV and you’ve multiplied the number of unverified things going straight into a vein.
How do I check out one piece of my stack before I add it in? Run the same checks on every single vial, not just the glutathione: was your history actually screened, is there a real prescription, can you name the licensed pharmacy, is sterility accountable to someone licensed, and is a qualified person actually reviewing the whole combination. Anything that fails screening, prescription, or sterility stays out of a protocol that includes an injectable. The documented harm here has consistently been sterility failures, not the molecule itself [5].
What exactly is a glutathione injection, and how’s it different from just taking a pill?
A glutathione injection puts the antioxidant straight into a vein or muscle, skipping your digestive tract entirely. Oral glutathione gets broken down in your gut before much of it reaches your bloodstream, which is why the absorption is so limited. Injections skip that whole step, so blood levels rise in a more predictable way. Whether those higher blood levels actually translate into meaningful benefits for an otherwise healthy person is still genuinely an open question.
Are these injections actually safe, or is that wishful thinking?
When a licensed compounding pharmacy makes it and a physician is supervising, glutathione injections have a reasonably solid short-term safety track record in clinical settings. The risk jumps way up with unregulated sources, contaminated vials, wrong pH, sterility failures, all documented causes of real harm. Even clean preparations can cause injection-site reactions, nausea, and occasionally more serious allergic responses. Injecting something you bought from a random website is a completely different risk category.
How much glutathione actually goes into a typical dose, and who’s deciding that number?
Doses used clinically and in research swing pretty widely, somewhere from roughly 600 mg up to 1,200 mg or more per session, depending on what it’s for. A prescribing physician should be the one setting your dose, based on your health, your reason for using it, and the specific formulation. There’s no universal “correct” amount, and dosing yourself off forum advice is genuinely risky since compounded products aren’t standardized from one source to the next.
Where does the injection actually go, and should I be doing this at home?
Clinically, it’s usually given IV or intramuscularly, with IV being the more common choice in wellness and functional-medicine settings. Home injection sounds convenient, but it comes with real downsides, bad IV technique can cause an air embolism, phlebitis, or a serious infection. If a physician determines this is right for you, going through a supervised compounding route like FormBlends keeps the actual preparation and the clinical oversight tied together instead of leaving you to sort it out alone.
References
- Witschi A, Reddy S, Stofer B, Lauterburg BH. The systemic availability of oral glutathione. Eur J Clin Pharmacol. 1992;43(6):667-669.
- Sinha R, Sinha I, Calcagnotto A, et al. Oral supplementation with liposomal glutathione elevates body stores of glutathione and markers of immune function. Eur J Clin Nutr. 2018;72(1):105-111.
- Aebi S, Assereto R, Lauterburg BH. High-dose intravenous glutathione in man. Pharmacokinetics and effects on cyst(e)ine in plasma and urine. Eur J Clin Invest. 1991;21(1):103-110.
- Glutathione for skin lightening: a regnant myth or evidence-based verity? Cureus. 2025.
- Johnstone P, Grace M, Doan B, et al. Acute systemic reactions following intravenous glutathione infusions. 2018.
- U.S. Food and Drug Administration. FDA warns compounders not to use glutathione from Letco Medical to compound sterile drugs.
Written by Uma Okafor, health explainer. Last reviewed January 2026.
Offered for general understanding, not as advice. Check with your provider before acting.